
The Problem
Children and youth with special healthcare needs (CYSHCN) and adults with multiple chronic conditions (MCC) represent the largest populations of high-need, high-cost patients.[2] CYSHCN and adults with MCC are common – they represent approximately 20% of all children and over 40% of all adults in the United States, respectively[3,4] – and despite their age differences, both groups share the common experience of frequently receiving fragmented, uncoordinated care.
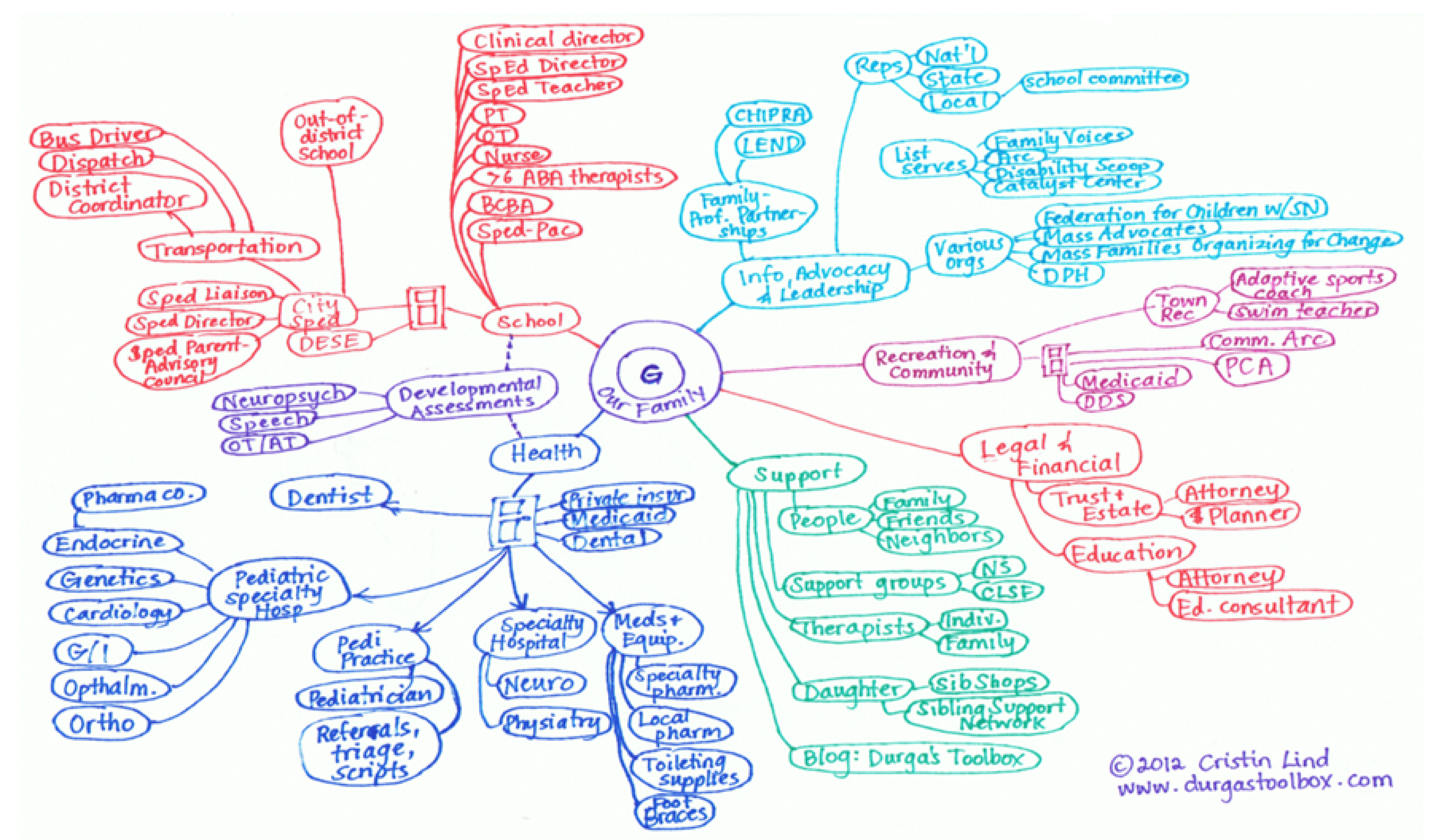
Care coordination interventions for CYSHCN[5] and adults with MCC[6] are associated with better health outcomes; however, many receive inadequate care coordination.[7] For example, a subset of CYSHCN have the highest health needs and costs[8] because they often have multiple chronic conditions, intensive home care needs (e.g., home health), functional limitations that impact daily living (e.g. reliance on a feeding tube), and require long-term multi-specialty follow-up.[9] As a result, their “medical neighborhood”[10] can involve a dizzying team of providers and health and social agencies (Figure 1). Parents/caregivers spend substantial time and effort – often >20 hours per week[11] – coordinating. Importantly, this is very stressful for families of CYSHCN as they are primarily responsible for care coordination ontheir own. The overall care experience is poor, leaving many families isolated and unsupported. One parentof a CYSHCN cared for at Duke shared that: “We, the parents, were the keepers of [his] lifelong medical chart… we were lay people, with a very complicated child, who was only growing more complicated.” This same stressful patient/family experience of fragmented, uncoordinated care affects adults with MCC and their loved ones. In order to reduce care fragmentation, improve the patient/family experience, and improve health outcomes, there is a critical need for better care coordination solutions for parents of CYSHCN and adults with MCC.
To manage a CYSHCN or adult with MCC’s lifelong medical record, patients and/or their families maintain extensive health records (e.g. history, procedures, medications) over time and across different health systems and providers in the forms of longitudinal care plans or paper binders.[12,13] However, such manually curated, often paper-based record keeping is time/labor-intensive and not synchronized with the electronic health record (EHR).
Our Solution
A personal health record (PHR) – a digital application through which parents can securely access, manage, and share their child’s health information[14] – would be transformative because a digital PHR: (1) accesses and organizes information across multiple health information systems (e.g., different EHRs); (2) includes parent/patient-reported information (e.g., care goals, symptom burden), and (3) facilitates transparent, bi-directional digital communication of PHR contents with providers.
A team of clinicians, developers, and family partners at Duke Health and Boston Children’s Hospital previously built a Fast Healthcare Interoperability Resources (FHIR)-enabled digital PHR mobile app called Caremap.[18] Caremap is an app to coordinate care for CYSHCN. However, FHIR-enabled EHR integration of the app as a care coordination solution in a real-world setting for CYSCHCN and adults with MCC is yet to be implemented.
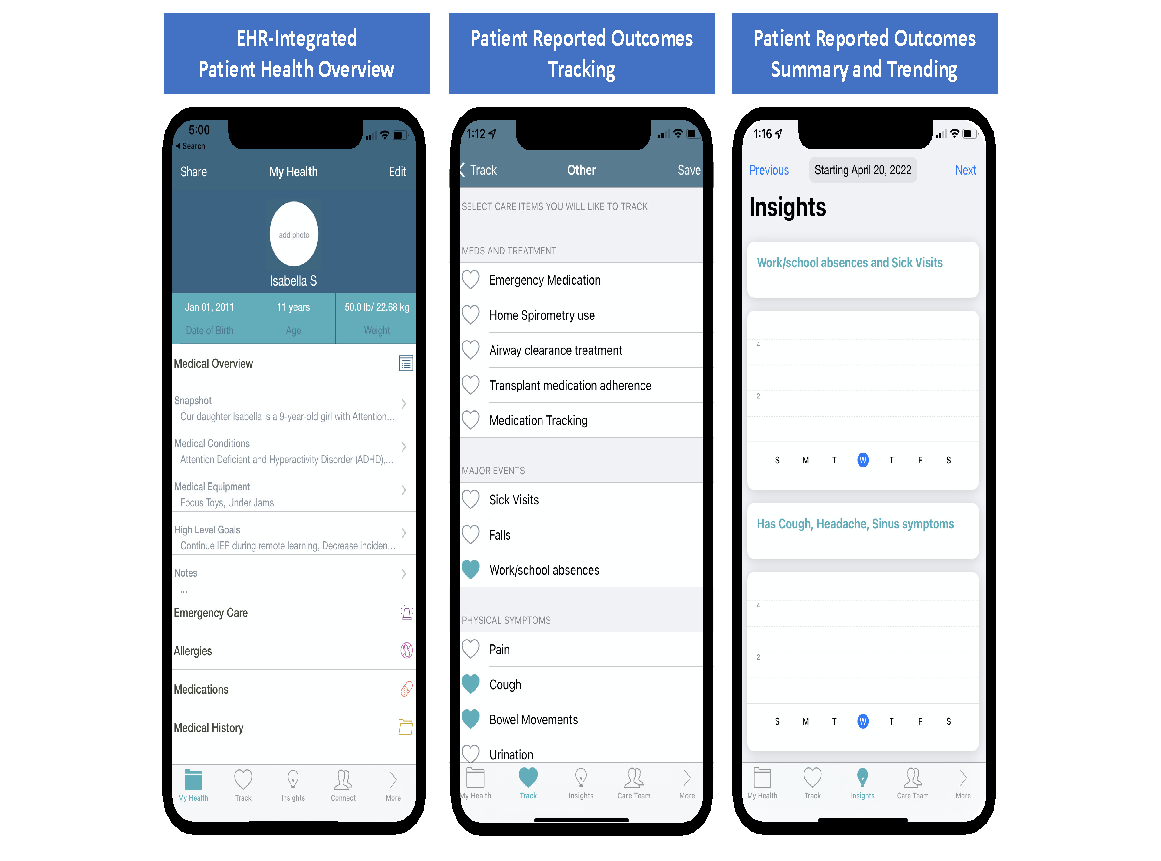
The Caremap mobile app leverages the Apple iOS© platform and can be used on Apple© personal devices (tablet, phone). The Caremap mobile app has three core features (Figures 2 and 3). First is FHIR- enabled access to structured data from the child’s EHR chart (e.g., medication list, allergies, problem list) and visualization of data within the app, thereby allowing patients/families to view the same health information seen by their Duke provider in the EHR. Second is a tracking feature so that patients/ families can track their progress towards patient- centered care goals (e.g., fewer missed school days due to illness, and adherence to routine medications).Third is a clinician dashboard that allows providers to visualize a summary of patient/ family-reported trends, progress, and insights within the EHR. These core features were co-designed with parents/caregivers and providers to tailor the app to best meet their needs. Previously conducted usability testing demonstrated proof-of-concept and strong support from families for Caremap as a promising digital health solution for care coordination.
We are live with the use of Caremap mobile app and have begun enrolling participants as of September 2022. To achieve our go-live with Caremap, we have completed significant activities in three core areas during the project period: embedment of participant recruitment within routine clinical workflows, information security, and technical development. This included exciting integration of the clinician dashboard with the mobile app and Epic© EHR via a partnership with a third-party platform (Xealth).
Furthermore, we completed the Duke School of Medicine and Duke Information Security Office (ISO) regulatory processes to ensure the security of data systems involved in the mobile app. This included meeting stringent review standards and comprehensive third-party penetration testing. Finally, we developed comprehensive study recruitment procedures and infrastructure using a novel digital prescribing process embedded within routine workflows. The digital prescription (‘e-prescription’) is a platform that leverages the EHR online patient portal (Epic MyChart©) to deliver all study-related materials – including onboarding materials (newly created video and written content), app download link, and informed consent – electronically directly to patients/families. Partnership with clinician champions in four Duke specialty care sites – two pediatric (pediatric pulmonology; neurodevelopmental pediatrics) and two adults (geriatrics; pulmonary transplant) – allowed the creation of workflows that will seamlessly integrate study recruitment and patient/family use of the app within clinical care at participating sites.

Impact
Our team’s experiences generated critical lessons learned that will be foundational information for other Duke innovators seeking to efficiently navigate the digital security review process with future EHR-integrated mobile apps.
We aim to enroll forty participants (ten participants per site) and gather prospective quantitative and user-reported data that will determine feasibility and impact of the mobile app on care coordination for CYSHCN and adults with MCC in specialty care settings.
Next Steps
We plan to collect qualitative data via semi- structured participant interviews in order to identify barriers and facilitators to implementation. We plan to complete the steps in the invention disclosure application process and have collaborated with internal and external partners to integrate the Caremap mobile app platform into interventions submitted for external grants.
Academic Output
We presented this study protocol as a peer- reviewed research abstract poster at the national Pediatric Academic Societies’ annual meeting in spring 2022. We have two peer-reviewed manuscripts in progress that were submitted for publication in fall 2022.
Special Thanks
These technical outcomes were made possible through extensive collaboration with multiple partners and groups internal (e.g., Digital Strategy Office; Duke Health Technology Services; Departments of Pediatrics, Medicine, and Population Sciences; Office of Research Administration) and external to Duke (e.g., Boston Children’s Hospital).
References
- Hospital BCs. Organizing Care and Relationships for Families: Care Map. http://www.childrenshospital.org/integrated-care- program/care-mapping. Accessed July 17, 2020.
- Blumenthal D, Chernof B, Fulmer T, Lumpkin J, Selberg J. Caring for High-Need, High-Cost Patients – An Urgent Priority. The New England journal of medicine. 2016;375(10):909-911.
- Musumeci MC, Priya Medicaid’s Role for Children with Special Health Care Needs: A Look at Eligibility, Services, and Spending. San Francisco, CA June 12, 2019 2019.
- Buttorff C RT, Bauman M. Multiple Chronic Conditions in the United States. Santa Monica, CA: RAND Corporation;2017.
- Council on Children with D, Medical Home Implementation Project Advisory C. Patient- and family-centered care coordination: a framework for integrating care for children and youth across multiple systems. Pediatrics. 2014;133(5):e1451-1460.
- Vasan A, Morgan JW, Mitra N, et al. Effects of a standardized community health worker intervention on hospitalization among disadvantaged patients with multiple chronic conditions: A pooled analysis of three clinical trials. Health services research. 2020;55 Suppl 2:894-901.
- Cordeiro A, Davis RK, Antonelli R, et al. Care Coordination for Children and Youth With Special Health Care Needs: National Survey Results. Clinical pediatrics. 2018;57(12):1398-1408.
- Cohen E, Berry JG, Sanders L, Schor EL, Wise PH. Status Complexicus? The Emergence of Pediatric Complex Care. Pediatrics. 2018;141(Suppl 3):S202-S211.
- Cohen E, Kuo DZ, Agrawal R, et al. Children with medical complexity: an emerging population for clinical and research initiatives. Pediatrics. 2011;127(3):529-538.
- Greenberg JO, Barnett ML, Spinks MA, Dudley JC, Frolkis JP. The “medical neighborhood”: integrating primary and specialty care for ambulatory patients. JAMA internal medicine. 2014;174(3):454-457.
- Kuo DZ, Cohen E, Agrawal R, Berry JG, Casey PH. A national profile of caregiver challenges among more medically complex children with special health care needs. Archives of pediatrics & adolescent medicine. 2011;165(11):1020-1026.
- Klitzner TS, Rabbitt LA, Chang RR. Benefits of care coordination for children with complex disease: a pilot medical home project in a resident teaching clinic. The Journal of pediatrics. 2010;156(6):1006-1010.
- McAllister JW, Keehn RM, Rodgers R, Lock TM. Care Coordination Using a Shared Plan of Care Approach: From Model to Practice. J Pediatr Nurs. 2018;43:88-96.
- Saripalle R, Runyan C, Russell M. Using HL7 FHIR to achieve interoperability in patient health record. J Biomed Inform. 2019;94:103188.
- Braunstein ML. Healthcare in the Age of Interoperability: Part 3. IEEE Pulse. 2019;10(1):26-29.
- Mandel JC, Kreda DA, Mandl KD, Kohane IS, Ramoni RB. SMART on FHIR: a standards-based, interoperable apps platform for electronic health records. Journal of the American Medical Informatics Association : JAMIA. 2016;23(5):899-908.
- Bloomfield RA, Jr., Polo-Wood F, Mandel JC, Mandl KD. Opening the Duke electronic health record to apps: Implementing SMART on FHIR. Int J Med Inform. 2017;99:1-10.
- Caremap. http://caremap.health/index.html. Published 2016. Accessed.


