
The Problem
More than 7 million people present annually to Emergency Departments (EDs) with symptoms of chest pain. (1, 2) Nearly 2% are misdiagnosed as NOT having an acute coronary syndrome and are discharged inappropriately; these individuals are at a markedly increased risk of death, myocardial infarction (MI) and other adverse cardiac events. (3) Conversely, of those admitted from the ED, only 10-20% are ultimately diagnosed as having an MI.(3, 4)
Improving the diagnostic accuracy in patients with chest pain would result in better tailoring of patients to treatment, fewer missed diagnoses, lower resource consumption, decompression of the ED, reduced liability, and better patient outcomes. Several tools have been validated in the management of the chest pain patient. (5) Specifically, the HEART score stratifies patients into low, medium or high risk for acute coronary syndrome, (6) and high-sensitivity cardiac troponin (hsTn) detects myocardial injury much more rapidly and with greater sensitivity than current 4th generation cardiac biomarker assays.(7-9)
The algorithm for interpretation of hsTn in the ED for the detection of myocardial injury requires knowledge of the duration of symptoms along with comparisons of the results of assays obtained at serial timepoints (0, 1 and 3 hours following presentation of the patient to the ED). The algorithm is based on a number of factors, including symptoms (< 3 hours versus >= 3 hours) as well as evaluation of both absolute and delta change of serial troponin levels. The algorithm contains numerous steps and decision nodes, demanding a substantial effort on the part of the clinician just to understand how the algorithm works, not to mention using the algorithm as a decision aid.
Our Solution
The Duke Chest Pain Assessment Tool (CPAT) is a more user-friendly way of integrating the clinical evaluation of the patient (represented via the HEART Score) and the serial hsTn cardiac biomarker assays into a clinical decision support aid.
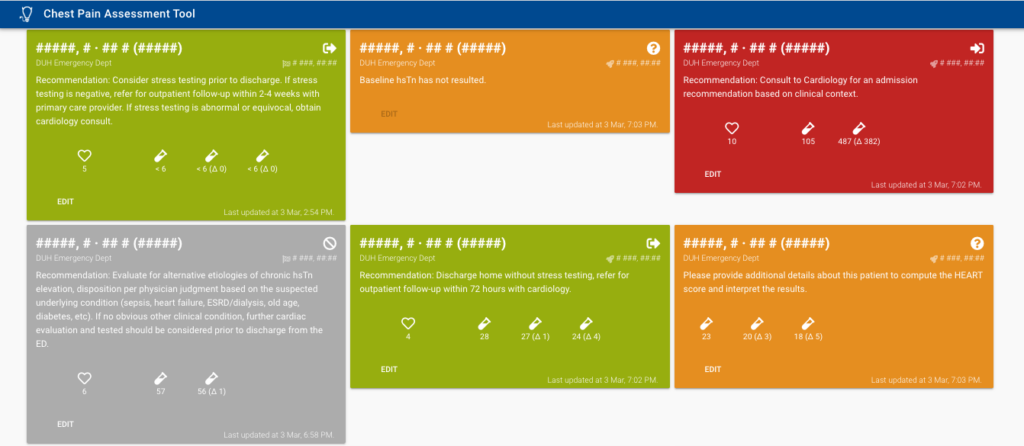
By leveraging FHIR, CPAT is able to retrieve information about hsTn orders to provide recommendations to ED Physicians based upon the hsTn interpretation.
1. Goodacre S, Cross E, Arnold J, Angelini K, Capewell S, Nicholl J. The health care burden of acute chest pain. Heart. 2005;91(2):229-30.
2. Nawar EW, Niska RW, Xu J. National Hospital Ambulatory Medical Care Survey: 2005 emergency department summary. Adv Data. 2007(386):1-32.
3. Pope JH, Aufderheide TP, Ruthazer R, Woolard RH, Feldman JA, Beshansky JR, et al. Missed diagnoses of acute cardiac ischemia in the emergency department. N Engl J Med. 2000;342(16):1163-70.
4. Body R, Carley S, McDowell G, Jaffe AS, France M, Cruickshank K, et al. Rapid exclusion of acute myocardial infarction in patients with undetectable troponin using a high-sensitivity assay. J Am Coll Cardiol. 2011;58(13):1332-9.
5. Than M, Cullen L, Reid CM, Lim SH, Aldous S, Ardagh MW, et al. A 2-h diagnostic protocol to assess patients with chest pain symptoms in the Asia-Pacific region (ASPECT): a prospective observational validation study. Lancet. 2011;377(9771):1077-84.
6. Six AJ, Cullen L, Backus BE, Greenslade J, Parsonage W, Aldous S, et al. The HEART score for the assessment of patients with chest pain in the emergency department: a multinational validation study. Crit Pathw Cardiol. 2013;12(3):121-6.
7. Reichlin T, Hochholzer W, Bassetti S, Steuer S, Stelzig C, Hartwiger S, et al. Early diagnosis of myocardial infarction with sensitive cardiac troponin assays. N Engl J Med. 2009;361(9):858-67.
8. Bandstein N, Ljung R, Johansson M, Holzmann MJ. Undetectable high-sensitivity cardiac troponin T level in the emergency department and risk of myocardial infarction. J Am Coll Cardiol. 2014;63(23):2569-78.
9. Shah ASV, Anand A, Strachan FE, Ferry AV, Lee KK, Chapman AR, et al. High-sensitivity troponin in the evaluation of patients with suspected acute coronary syndrome: a stepped-wedge, cluster-randomised controlled trial. Lancet. 2018.


